Dupuytren’s contracture
 The Basics
The Basics
Dupuytren’s disease, or Dupuytren’s contracture, is a condition of the hand in which the fingers flex and “contract,” or permanently curl into the palm. Dense nodules underneath the skin and pitting of the skin can also be present. The small finger and ring finger are most commonly affected, but any part of the hand can be involved.
As this disease progresses it becomes more difficult to extend the fingers and flatten the hand, making simple tasks like shaking hands, washing one’s face, or even reaching into a pocket, difficult if not impossible. Usually Dupuytren’s disease is painless.
Who was Guillaume Dupuytren?
Dupuytren’s c ontracture is named after the famous French anatomist and military surgeon Guillaume Dupuytren (1777-1835). Dupuytren was a medical prodigy. By age 20 he was appointed assistant surgeon at Paris’ Hôtel-Dieu. He developed one of the largest and most respected practices in all of Europe. His ability to diagnose and heal others earned him great fame and fortune. By all standards, he was a celebrity. He published articles describing contracture of the palmar fascia, as well as treatment techniques. In 1816 he was appointed head surgeon at Hôtel-Dieu, a position he held until his death.
ontracture is named after the famous French anatomist and military surgeon Guillaume Dupuytren (1777-1835). Dupuytren was a medical prodigy. By age 20 he was appointed assistant surgeon at Paris’ Hôtel-Dieu. He developed one of the largest and most respected practices in all of Europe. His ability to diagnose and heal others earned him great fame and fortune. By all standards, he was a celebrity. He published articles describing contracture of the palmar fascia, as well as treatment techniques. In 1816 he was appointed head surgeon at Hôtel-Dieu, a position he held until his death.
Interestingly, Dupuytren’s contracture was not originally described by Guillaume Dupuytren, but rather by the Swiss physician Felix Plater (1536-1614). Plater described this contracture of the hand in 1614, nearly 150 years prior to Dupuytren’s birth.[i]
Terminology
- Dupuytren’s Contracture: a fixed flexion deformity of the hand due to contracted palmar fascia
- Dupuytren’s Disease: the same as Dupuytren’s Contracture
- Dupuytren’s Diathesis:
- a more severe form of Dupuytren’s disease
- presentation at a younger age (20s or 30s)
- aggressive cord involvement
- frequently multiple digits
- often bilateral (both hands affected)
- may have foot and/or penile involvement
- higher recurrence rate after surgery
- more involved rehabilitation after surgery
Pathology
Cells called myofibroblasts are responsible for the development of these contractures. Myofibroblasts reside within the tissue just beneath the palmar skin in a layer of tissue called “fascia” or “aponeurosis,”
Who gets Dupuytren’s disease?
Dupuytren’s disease is seen most frequently in men (the male:female ratio is 7:1) over 60 years of age, usually with northern European, British, or Scandanavian ancestry. The disease presents much less frequently in women, and when women are affected the disease progression is often atypical. The gene for Dupuytren’s is inherited as an autosomal dominant trait.
What are the symptoms of Dupuytren’s disease?
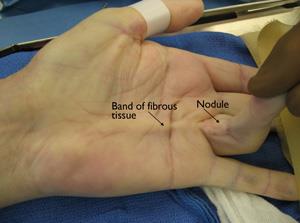
Dupuytren’s disease usually presents as a painless nodule or cord in the palm of the hand, most often in line with ring finger or small finger. Pitting of the palmar skin can also be seen. Over time the contracture becomes more severe, and the fingers begin to curl into the palm. Eventually the patient cannot flatten the hand on a level surface (such as a table), and performing simple tasks that require grasping and opening the hand become impossible.
Treatment
Dupuytren’s contracture is a complex hand condition that should only be treated by a trained hand specialist. With recent advances in technique and pharmacology, there are now several options to consider when treating Dupuytren’s disease.
Traditionally, Dupuytren’s contracture has been treated surgically by excising the cords and nodules in what is called a “palmar fasciectomy.” The surgery requires a high level of expertise to perform. Risks are rare, but include nerve, artery, and tendon damage, as well as the occasional need to skin graft some regions of the hand at the end of the procedure. Results can be very good to excellent. The procedure is usually performed as outpatient surgery, and takes about 1-2 hours, depending upon the severity of the contracture. Afterwards a splint is worn full time for 4-6 weeks, and then only at night for 4-6 weeks. Hand therapy after this procedure is common.
Needle aponeurotomy (NA) is a newer, less invasive approach to treating Dupuytren’s contracture. This technique can be performed in the office or outpatient surgery center using local anesthesia. NA uses a small hypodermic needle to divide the palmar cords and straighten the finger. This procedure takes less than a half hour. Afterwards a splint or soft dressing may be applied, based upon your surgeon’s preference. The need for hand therapy after this procedure is variable, depending on your surgeon. Risks are rare, but include nerve and tendon damage. Again, results can be excellent, and the procedure is quick and relatively inexpensive.[ii]
The injection of collagenase (brand name: Xiaflex, manufactured by Auxillium Pharmaceuticals) is the latest technique in treating Dupuytren’s contracture, recently gaining FDA approval. Collagenase is a chemical that breaks down the collagen structure within the palmar cords. In the doctor’s office, collagenase is injected directly into the palmar cord. Over the next 24 hours the cord breaks down, and the following day the patient returns to the doctor’s office for manipulation of the injected joint. Like NA, splinting and hand therapy depend upon your doctor’s preferences. Risks include tendon damage. Results can be excellent.[iii]
Because the proclivity for the hand to contract is “hard-wired” in the myofibroblast’s cellular DNA, the only way to truly eradicate Dupuytren’s disease would be to alter one’s genetic code. Until gene modification is achieved, the risk of recurrence at 3-5 years is high in all three of the above procedures. Comparative studies show that at 5 years Dupuytren’s contracture treated surgically has a lower recurrence rate than if treated with either NA or collagenase. [iv]
Conclusion
Surgical treatment, needle aponeurotomy, and collagenase injection each have specific risks and benefits. You and your hand specialist will determine the best course of action to meet your individual needs.
If you think you have Dupuytren’s contracture please call the hand specialists at WOSM to schedule an office examination.
[i] Benson LS. Dupuytren’s contracture. J Am Acad Orthop Surg. 1998;6:24-35.
[ii] Eaton C. Percutaneous fasciotomy for Dupuytren’s contracture. J Hand Surg Am. May;36(5):910-5.
[iii] Gilpin D, et al. Injectable collagenase Clostridium histolyticum: a new nonsurgical treatment for Dupuytren’s disease. J Hand Surg Am. Dec;35(12):2027-38.
[iv] Van Rijssen AL, Ter Linden H, Werker PM. 5-year result of randomized clinical trial in Duputren’s disease: percutaneous needle fasciotomy versus limited fasciectomy. Plast Reconstr Surg, 2011.